Part 12
The days following our meeting with Dr. Carnovale seem to SLOWLY pass by. I find myself counting the days until we “start” IVF. And by “counting down the days”, I mean counting down the days until May 1st. Up until this point, I have NO information about the IVF process except what a quick Google search will provide. I know there will be shots. I know there will be pills. I know there will be mood swings and night sweats and weight gain and weight loss and food cravings and a loss of appetite – but that’s about all I know.
I keep wondering, “what the hell is going on?!?!” My Type A personality can’t take all the “unknowns”. I am a planner. I need information!
About a week after my appointment with Dr. Carnovale, I get a call from Sarah – with information (praise the Lord). She tells me that I need to attend a “class”. The class is held on April 16th from 12:30 p.m. until 3:30 p.m. In that class they will go through all of the information related to the IVF process, including the medicines, injections, the calendar, etc.
I ask, “Do I need to bring Ben with me?”
Sarah says, “Only if he will be giving you the injections, otherwise it’s not necessary for him to be there, but he is more than welcome to come. A lot of men come and a lot don’t.”
Question answered. Ben’s busy and taking off a half-day of work to attend a class that he may or may not need to be at seemed pointless. So I told him to stay home. He was fine with it. I think the office stresses him out. Besides, Ben’s idea of “helping” with the injections is closing his eyes and looking away so he doesn’t pass out or vomit. Helpful, I know.
So, with new information in hand, I begin counting down the days until what I am lovingly referring to as, “Getting Pregnant School”.
When April 16th arrives, it feels like just another day. I work in the morning from home, then shower and put on some “normal human cloths”. For those of you who work regularly from home, you know that there’s no need to shower and put on clean cloths if you don’t have to leave the house. I prescribe to that mantra regularly. Today, however, I should look human.
I get in the car at about 11:45 a.m. to head to Dr. Carnovale’s office – knowing with that amount of time, I’ll still be 10 or 15 minutes early. I pull into the parking lot of his office with 20 minutes to spare, so I sit in the car for a few minutes before I head in. I walk into the building, it’s an all glass, 3-story atrium building with a staircase and elevator in the middle. Dr. Carnovale’s office is in the back corner of the third floor. His office has an all glass front and a solid glass door at the end of a lengthy hallway. When you turn the corner to go down the hallway to his office, you can see the entire waiting room. I take the stairs up to the third floor. As I round the corner into the hallway to his office, I almost stop dead in my tracks. What I see, at the end of the hallway, is a waiting room full of husbands and wives, sitting, not talking.
I immediately think, “Crap. I should’ve brought Ben with me.” I walk down the hallway and I feel all the women sitting in the waiting room staring at me as I walk down the hall. I grab the door handle and walk in. The room is silent. Silent in an awkward way. The waiting room only has 12 chairs in it. There are five husband and wife couples sitting there in complete awkward and uncomfortable silence. I come in, wave to Jodi and sit in one of the two empty seats. I pick up my phone and immediately text Ben, “I should’ve made you come with me. You’re the only husband not here.”
I’m not worried about it – I just feel bad for Ben. Perhaps this is something he needs to hear. I stare up at the TV because that’s what everyone else is doing. Fox News is on – ugh. Something ridiculous is said, and I make an under breath comment to the women sitting next to me. She looks at me blankly then looks away – as to say “don’t talk to me”. The awkward silence in the room is so tense I can’t take it. I look around the room and everyone is staring at me with a look like they’re thinking, “you’ve got some nerve making noise, much less thinking we’re interested in engaging with you.” I don’t know if I have ever been so uncomfortable in my entire life.
So I do the only thing that is socially acceptable to do in that room. I pull out my cell phone and check Facebook. This. Is. Awful.
Ten minutes later, Sarah comes in and gives us a brief overview of what’s going to happen. She says, first, we are going to be having Dr. Carnovale’s resident psychologist come in to talk. Then she’ll be going through the IVF schedule, medicines, and teaching us how to do the injections. Finally, we’ll hear from Dr. Boldt, the embryologist about his process and what to expect. Okay, I can handle this. I still don’t understand how this is all going to take 3 hours though, but okay. I’m along for the ride. At least there will be something to break the silence.
First the psychologist comes in…
Keep in mind that I have several very close personal friends that happen to be mental health advocates, most of them speakers on mental health and all of them have worked at one point in their career, full time in mental health advocacy. I know the language. I know about how they erase stigma associated with mental illness. I know the formula for building rapport and trust with people – I teach it for a living. So when the psychologist sits down, introduces herself, and immediately launches into her personal story of infertility – I about lose my shit. For someone as well informed as I am about the method behind exactly what she is doing – it almost feels like she’s antagonizing me.
I know what the hell you’re doing lady. I see right through it. You’re not fooling me.
Her spiel is short (thank goodness) and she leaves. I feel my blood pressure lower immediately. I have no idea what she said, except “blah blah, it’s going to be hard. Blah blah support each other. Blah blah, I’m hear to talk to you when you need it.” Yeah, yeah, yeah.
Sarah then walks in with a mountain of supplies and a stack of folders. She proceeds to hand each of us a very specific folder. She passes mine to me. It’s thick. I open it and begin thumbing through the pages. On one side of the folder theres a calendar with “May” written at the top. Each day is filled with appointments, medication dosages, and instructions. Behind it are about 10 sheets of paper each with a different medication name on it: Cetrotide, Menopure, Follistim… Beyond that are pages that say “Subcutanous (Belly) Shot Instructions” and “Intramuscular (bottom) Shot Instructions”. As I scan each of these pages there are lengthly step-by-step mixing instructions, how to draw the medicine from the vial, which needle and syringe to use, etc. I am already overwhelmed.
On the other side of the folder is 30 pages of consent forms for the IVF process. What should we do with the embryos if you die? What should we do with the embryos if your partner dies? What should we do with the embryos if you both simultaneously die? What should we do if you get divorced? How should we fertilize the egg? Do you want us to freeze the leftovers? What if you decide to stop IVF and we have frozen eggs? Will you donate them to science? What type of science can we use them for? Do you want us to dispose of them? How should we dispose of them? All of the pages have to be signed and notarized. Notarized. This is serious. There’s a thousand questions we have to answer and discuss and have notarized by our first appointment on May 2nd.
Oy. My head is spinning.
In my daze I hear Sarah’s voice, “Okay everyone, on the left side of your folder there should be a calendar, let’s go through that first.”
Sarah then begins to go through, day-by-day the instructions for the IVF cycle. First, Ben and I have to take 10 days worth of antibiotics, starting April 24th. April 26th is my first injection – it’s Follistim, a follicle stimulating hormone.
For my friends who, like me hadn’t paid much attention is the “period” class we took in 6th grade nor the biology class we took in 9th grade, I had no idea what she was talking about. Eggs are released from the ovary through follicles. For most women, they produce one follicle each month. They’re like little sacs of fluid that form on the outside of the ovary where the egg sits and matures. On the day of ovulation, the follicle bursts and the egg releases – beginning it’s trek down the fallopian tube. In fertility patients, they stimulate you so that you body produces multiple follicles so they can get multiple eggs to fertilize.
This medicine, Follistim, has a pen – it’s actually pretty simple. You screw on the needle, that’s already in a nice little package, dial up the dosage, stab yourself and you’re done. Sarah passes out a pen and a needle to everyone and we practice putting on the needle, dialing up the medicine, and pushing the plunger to get the medicine out (it’s not real medicine, just saline considering that just 300 IUs of the medicine costs $500)
The next medicines require mixing. Sarah takes her time showing us with the actual needle and syringe how to mix the medicine in the vial, swirling slowing as to not create bubbles and then drawing the medicine into the syringe again.
There’s several more medicines that she shows us how to mix, some that are on my list, some that aren’t (there’s a variety of reasons women need fertility treatment, thus a variety of drugs that one might have to take dependent on what is the “factor” for infertility).
From there, Sarah has us turn to the pages regarding how to give the injections. She begins by asking, “So gentlemen, this is where you come in. Jessica, you’ll just want to be sure you walk Ben through how to give you the injections.”
Wait what?
I respond, “Oh, I’m giving them to myself.”
Just then I see and feel the piercing eyes of every man and woman in the room. I didn’t know there was going to be judgement about me giving shots to myself. Frankly, my Type A tendencies can’t stand the thought of someone else injecting me. I have to look away when I get blood drawn – not because I can’t stand to see the blood or the needle – but because I can’t stand to think about the incompetence of the person drawing my blood, I can’t watch the train wreck happen.
Sarah begins with the “belly shot”. This one seems relatively easy. Pinch some of the skin at or around your belly button (for Sarah it’s skin – she’s rail thin) for every other human being, it’s a nice hunk of belly fat. Pinch the fat, clean the area with an alcohol swab, hold the syringe like a pen, and with a dart-like motion, stab the syringe in, and depress the plunger. I can do this…maybe.
Sarah then turns to the “bottom shot”. Sarah begins, “This shot has to go into a thick muscle mass. You can choose your bottom or your thigh. If you were to divide your butt into four quadrants, the target area is the upper-outer quadrant. While bending slightly at the hip, pigeon-toed (to relax the muscle), choose a section of the skin and pull it taut. Clean the area with an alcohol swab. With a dart like motion, stab the needle in. Before depressing the plunger, pull the plugger back to see if you draw any blood into the syringe. If there is any blood, you’ve hit a blood vessel. Pull the needle out and try a different spot. If no blood, slowly depress the plunger. Apply pressure to the injection site immediately.”
Sarah continues, “The only medicine you will be injecting as a “bottom” shot is Progesterone. This medication is in oil. Because you are injecting oil into a muscle mass, it will likely cause some pretty intense muscle soreness and bruising. We recommend you ice the area before and after the shot. In fact most of the injections you might notice some bruising. It’s perfectly normal. If anything begins to get inflamed call us immediately.”
“Lastly,” Sarah says, “You need to keep track of how much of each medicine you have and you need to carry your calendar with you at all times. We could call you at any moment and adjust your dosages or schedule. When you come in, we will ask you how much medicine you have left so we know if we need to order more.”
Okay, any questions? Silence. Everyone in the room is awkward and afraid to speak. I obey the laws that that have clearly been set by the other women in the room and keep my mouth shut.
Sarah then says, “Okay then. Let’s draw our attention back to the calendar. You will all begin injections on April 26th. On May 2nd is what we call your “baseline appointment”. On that day you will come in and Dr. Carnovale will do an ultrasound to look at your ovaries. If you have any cysts, you won’t be able to continue with this month’s round. You’ll have to wait. Most cysts resolve themselves after about 1-2 months. Then you can resume. Sometimes this happens and it’s hard to deal with, but you just have to wait a little while longer. Next you’ll see…”
Wait. That seems like something pretty major to just breeze over. A cyst? Crap. A cyst can cause a delay. I hope I don’t have a cyst. It didn’t seem like a big deal to Sarah, so I don’t worry about it.
“…next you’ll see that about every other day we will need you to come in. We will do an ultrasound and take some blood to test your hormone levels. After about May 9th, all bets are off. You’re body could be ready for egg retrieval at any time after that. The doctor could want to see you on a Saturday. He could schedule your retrieval on a Sunday. It’s all dependent on your body. You need to be ready for anything that comes. We have no way of predicting how it will all play out.
When you are ready for egg retrieval, you will be given instructions for your HCG shot. This shot has to be taken at the VERY PRECISE TIME that we give you. Not a moment before or after. This shot will cause your eggs to finish maturing and release from the ovary. We schedule the retrieval so that the eggs have matured, but not released yet. If you get into the egg retrieval and the eggs have already released from the follicles, we can get them – and you’ll have to start over…”
Okay I am sufficiently scared. Let’s move on.
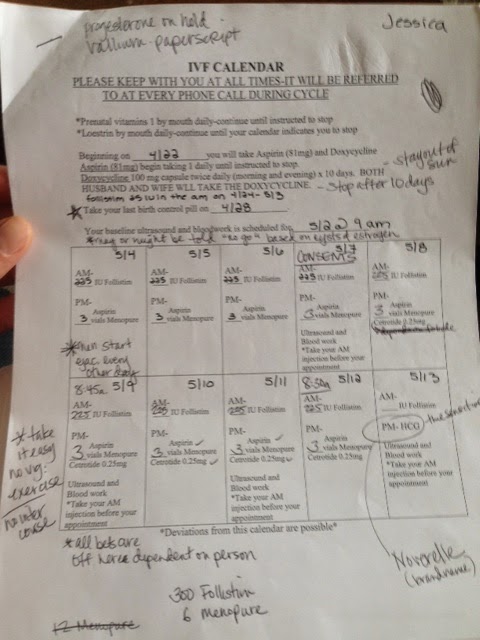
“…You’ll come into the hospital the next day for retrieval after your HCG shot. You’ll be under anesthesia for retrieval. It takes about 45 minutes. You’re husband will also have to supply a sample that day for fertilization. If you notice on the calendar on May 9th, we need the husbands to begin ejaculating every other day, beginning the 9th. For you ladies, beginning on the 9th you are on activity restriction. No exercise, no sex, no heavy-lifting. You can only walk.
I chuckle to myself and think, “Sorry Ben-bo, you’re on your own. LOL.”
“After egg retrieval, Dr. Boldt, who you’ll meet here soon, will call you every morning with an update on your eggs. When they are ready to be implanted (between 3 and 5 days after retrieval), you’ll come back into the hospital. They’ll implant the embryos and you’ll be on bed rest for two days. After that no lifting more than 5 pounds or any exercise until your pregnancy test. We want you to take it VERY EASY until the pregnancy test, which is two weeks after retrieval. Do me a favor, during that two weeks – STAY OFF THE INTERNET. The Two Week Wait (or as online forums call it 2WW – I don’t follow instructions well) is really hard already, don’t make it worse by going online into the fertility support groups. Do not do the home pregnancy tests either. You have too many hormones pumped into you for them to be accurate. You only have to wait two weeks, then you take a blood pregnancy test. That is the most accurate way for us to determine pregnancy.”
Sarah then smiles, perks up in her chair and says, “Then you’ll hopefully be pregnant. Any questions?!?”
Silence. I have a thousand questions. For one, this is really complicated what if this? What if that? What do you mean no activity? What about this? What about that? But the awkward silence in the room keeps me from speaking.
Dr. Boldt then walks into the room. He’s a tall, stalky, older Scandinavian looking gentleman. He’s warm and funny and I immediately feel at ease with him in the room. He then launches into the most illuminating education on embryology I’ve ever had with pictures and statistics and all. I write down every word. This percentage of this and this percentage of that and this and that. I start looking at the percentages and getting really scared. 70-75% of follicles have an egg in them. 80-85% of the eggs fertilize. 90% of fertilized eggs divide into embryos. 50% of those embryos get to the “blastocyst” stage (the stage where they are a viable option and are likely to implant in a woman’s uterus). 50-60% of all cases they have extra embryos to freeze.
When you do that math, my projected 5 eggs (from my Ovarian Reserve Test) whittle down to very few viable options left. The realist in me starts to worry. I am quickly distracted however, by Dr. Boldt’s claim that he can get from his house at 146th and Springmill to the hospital in 8 minutes. No way. He an I break the awkward silence in the room and start arguing in witty banter. I like him.
Just then Sarah walks into the room and Dr. Boldt says, “Alright everyone. We’ll be seeing you soon. Good luck.”
Sarah then says, “If anyone has any questions, I stick around and answer them.”
I look down at my watch and it’s 3:30 on the dot. Wow. That really did take 3 hours.
I dump everything in my bag and bolt out of the room. There’s no way I’m waiting in line with all those women to talk to Sarah. I just call the office tomorrow. I have a thousand questions. Mostly I am just really really afraid that this isn’t going to work.
I get down to my car, toss my stuff in the passenger seat, buckle my seatbelt and begin to sob.
I’ve never been so scared in my life.
